BLEPHAROPLASTY SURGERY AND ALTERNATIVE TREATMENTS
The effects of aging, sun damage or certain conditions such as angioedema (intermittent swelling of the eyelids) can result in the development of excess skin on the upper eyelids resulting the tired or heavy appearance that patients seeking upper eyelid surgery often describe.
In addition to the development of excess skin the internal structures of the upper lid can weaken over time (as part of the ageing process and because of other additional factors) leading to the fat that surrounds the eyeball bulging forwards from the eye socket into the eyelid causing a ‘puffy’ appearance.
Eyebrow position is a further factor that impacts on the look of the upper eyelid - as the position of the eyebrows lower over the course of a lifetime the skin directly beneath the brow drops like a roller blind onto the lid exacerbating any inherent skin excess producing an even more hooded appearance to the upper lid.
Patients often report these changes have a negative effect on their levels of self-esteem and psychological wellbeing.
The aim of the surgery is to reduce the amount of skin on the upper lid and correct any bulging of the soft tissues from the eye socket into the eyelid. Eyelid surgery will not affect brow position and if some of the skin excess on the lid is due to ‘roller blind’ effect of the skin below the eyebrow, then the hooded appearance of the eyelid may not be fully corrected. This is something that your surgeon will discuss and advise you about (you may require a brow lift in addition to blepharoplasty surgery in order to achieve your desired aesthetic outcome).
Blepharoplasty surgery, as with all cosmetic surgery procedures aims to produce a psychological benefit for those undergoing surgery as well as improving the appearance of the face. As with any cosmetic procedure it is important to have realistic expectations about the results.
HOW IS UPPER LID BLEPHAROPLASTY SURGERY PERFORMED?
There are multiple techniques that can be used when performing upper-lid blepharoplasty surgery although there are usually common components:
• redundant skin excision
• removal or repositioning of any soft tissues protruding from the eye socket (orbit) into the eyelid
As with most surgical procedures dealing with rejuvenation of appearance, the aim of the surgery is to restore the anatomy of the eyelid as close to the state that would have been seen in an individual’s youth. It is never going to be possible to restore that exact appearance but the goal of the procedure is to improve the look of the eyelid (by addressing these changes).
Although the actual amounts of skin removed vary from individual to individual, there are some general anatomic landmarks that are used by surgeons as a guide during the procedure:
• the eyelid crease (known as the supratarsal crease) that is used to mark to mark the lower incision margin (this is usually somewhere between 8 and 10mm above the eyelashes)
• a line below the lower margin of the eyebrow that can is placed at a variable distance from the lower border of the eyebrow but that usually keeps 10mm of skin intact below the brow.
As with all operations, the exact manner in which it is performed is tailored to the individual. Your surgeon will discuss with you which technique they believe will work best in your case and with a view to accommodating or best meeting your own aims.
It is not usual for a surgeon to explain in detail every possible technique but if you wish to discuss that in further detail/obtain further information please ask your surgeon.
If there are particular goals you wish to achieve from the surgery then you need to make sure that you have discussed these with your surgeon so that they can discuss the options available to best address them.
ADDITIONAL FORMS OF TREATMENT
In certain circumstances an improvement in eyelid shape can be brought about by increasing the volume of the soft tissues below the eyebrow (usually in individuals with a hollowed-out appearance to their upper lids). This can be done by fat grafting (taking fat from another site on the body and injecting it into the facial tissues).
In certain circumstances improvement in brow position alone may restore the youthful appearance of the upper lids (when skin excess on the upper lid is the result of the ‘roller blind’ effect from brow descent).
Skin tightening can be produced by the use of energy transfer devices (such as plasma, laser or radiofrequency).
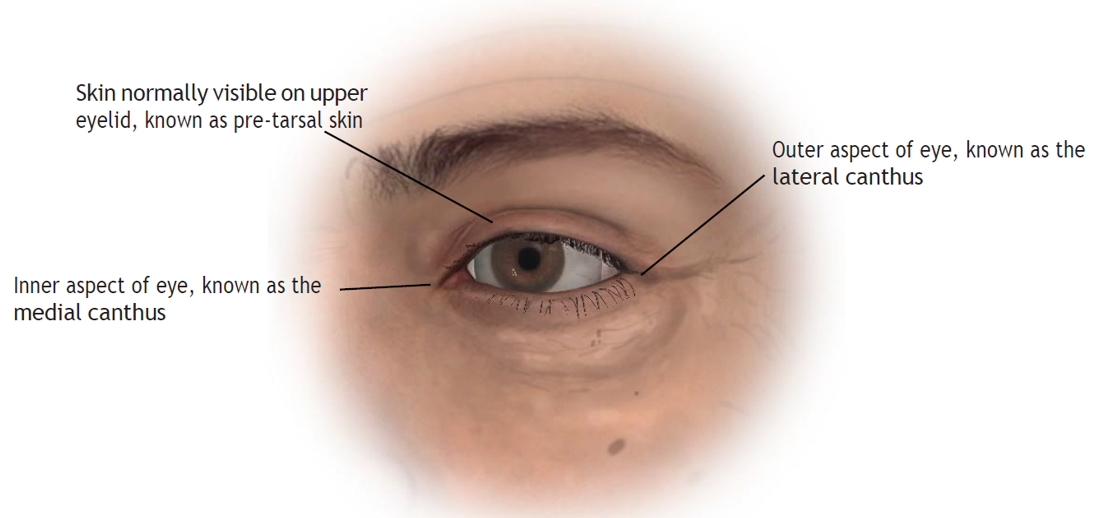
Illustration (upper eyelid, unaged appearance):
The youthful upper eyelid is characterised by a clearly visible strip of eyelid skin directly above the eyelashes. This is known as the pre-tarsal skin (so called because lying beneath the skin is a structure called the tarsal plate made out of tissue similar to cartilage, which gives the margin of the eyelid substance). The upper boundary of this area of skin is called the supra tarsal crease (it is formed by fine ligaments running from the top of the tarsal plate into the eyelid skin) above which the skin continues up to the eyebrow in a slightly con- cave fashion. The inner and outer margins of the eye (where the medial and lateral margins of the upper and lower tarsal plates attach into the bone of the orbit) are called the medial canthus and lateral canthus
respectively.
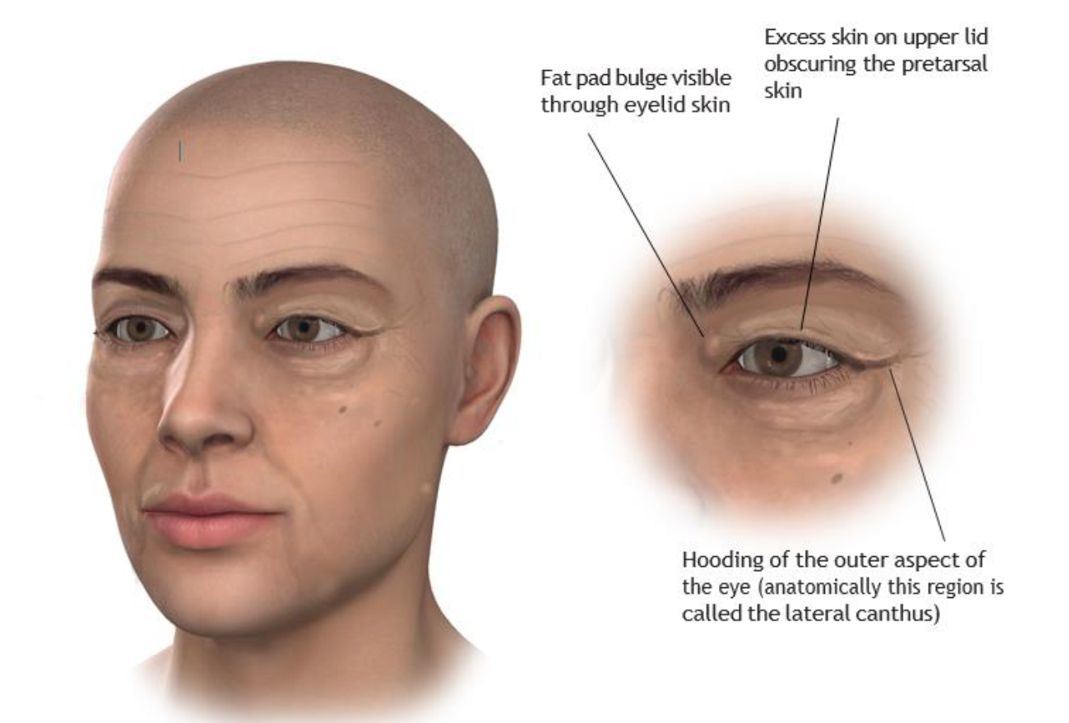
Illustration above (upper eyelid changes seen with age and typical upper eyelid blepharoplasty incision):
Top left: Global changes seen in facial aging including deepening of the nasolabial folds, marionette lines and development of excess skin around the eyelids and the development of eye bags.
Top right: Typical appearance of the aged upper lid. Excess skin on the lid (often due to a combination of true lid skin excess and the secondary effect of brow descent ‘shuttering’ additional skin onto the lid) obscures the pre-tarsal skin above the lashes. Weakening of the orbital septum (please see diagram on page 6) allows fat to bulge forward from inside the eye socket (orbit) resulting in a ‘puffy’ appearance to the upper lid. The outer aspect of the eye is hooded as a result of skin excess and brow descent, this can impact on peripheral vision.

Top left and right: Typical incisions for an upper lid blepharoplasty. The area shaded in blue represents the skin that is usually removed as part of an upper lid blepharoplasty. Depending on the technique employed by your surgeon the muscle directly underlying this skin may also be removed. The black arrows beneath the eyebrow denote the extent of skin that needs to be preserved as part of the procedure (this is normally a minimum 10mm) whilst the white arrows demonstrate the area of pre-tarsal skin that is preserved (this varies between men and women and is usually sited at the level of the supra tarsal crease).
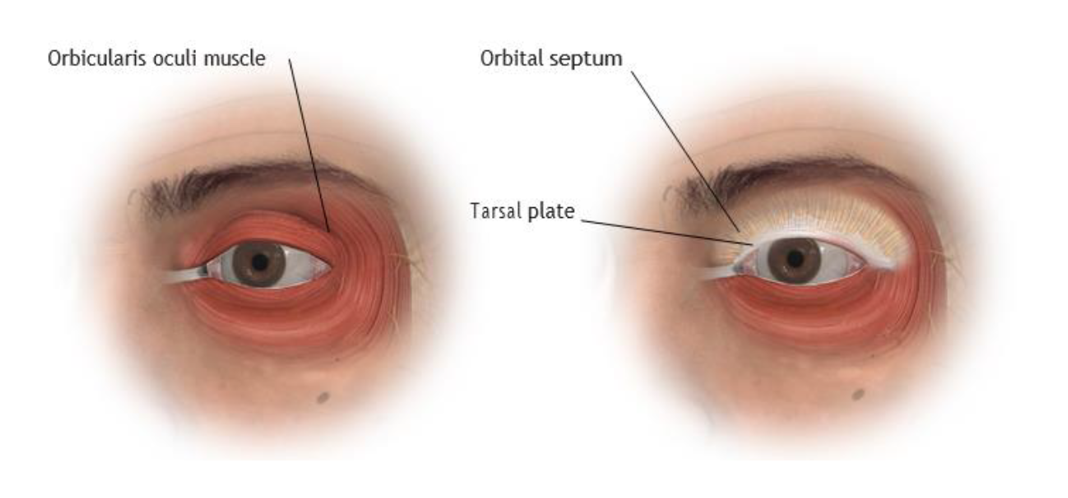
Illustration (upper eyelid anatomy):
Top left and right: The layer beneath the skin is the muscle that is responsible for closing the eye, known as the orbicularis oculi. It covers the eyelids and the bone of the eye socket. Beneath the orbicularis muscle is the orbital septum and the tarsal plate. The tarsal plate gives the eyelid margin shape and structure and con- forms the lid to the shape of the globe (eyeball). The orbital septum is a thin sheet of connective tissue arising from the edge of the tarsal plate which inserts into the margin of the eye socket. Its job is to protect the con- tents of the eye socket and keep the fat surrounding the eyeball in the eye socket.
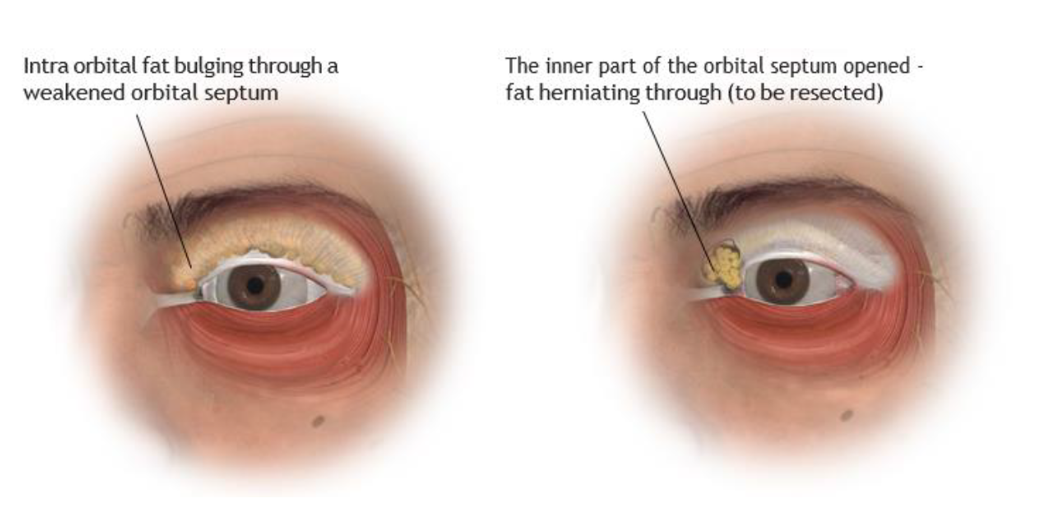
Illustration: Top left and right: With age the orbital septum weakens and stretches allowing the fat from within the eye socket to bulge forward producing the familiar puffy appearance to eyelid. During an upper lid blepharoplasty the orbital septum is opened and any fat that bulges through is trimmed off to correct the puffiness within the eyelid.
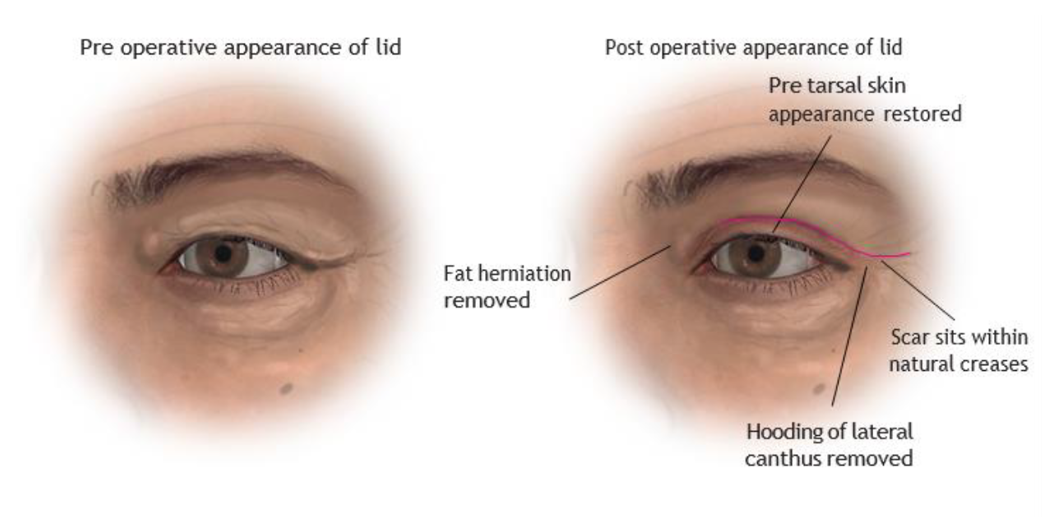 Illustration above: Comparison of pre and post operative appearance of the upper eyelid. The ageing features of the upper lid are removed, restoring a youthful appearance. The scar sits within the natural skin creases of the upper lid.
Illustration above: Comparison of pre and post operative appearance of the upper eyelid. The ageing features of the upper lid are removed, restoring a youthful appearance. The scar sits within the natural skin creases of the upper lid.
WILL THE RESULTS OF SURGERY BE PERMANENT?
It is important to appreciate that the result of any upper lid blepharoplasty procedure is dependent on not only treatment of lid anatomy but also restoration of brow position. As we age, the position of our eye brows drops (every time you look at bright light think of how you squint, partially closing your eyes and pulling your eyebrows down to act as a sun visor, over a lifetime this stretches the soft tissues and the eye brows end up in a lower position on the forehead). Therefore, although the skin (and other soft tissues) in the upper lid may have been adequately treated it can appear that excess skin on the upper lid has reaccumulated (when in fact it is the skin beneath the eye brow that is producing the hooded appearance to the upper lid).
Under normal circumstances it is unusual for excess skin to recur on the upper lid after having been addressed with an upper lid blepharoplasty (as with everything there are exceptions to this observation, usually relating to medical conditions associated with collagen deficiency or recurrent eyelid swelling).
In addition to above mentioned conditions that can produce recurrence of skin on the upper lids there are a few rare medical conditions that can cause a change in appearance of the eye and eyelids because of swelling of the soft tissues inside the eye socket; the most common one encountered is the result of changes in thyroid gland function.
Having realistic expectations and an understanding of the balance struck between lid skin and eye brow is essential before undergoing upper lid blepharoplasty surgery.
HOW UPPER LID BLEPHAROPLASTY IMPACTS ON OTHER STRUCTURES
As mentioned earlier in the booklet surgical treatment of excess skin on the upper eyelid can result in changes to the position of other structures in the orbit and forehead:
Eyebrow shape and position: The position of the eyebrows has a direct relationship with the amount skin present on the upper eyelids. When excess skin accumulates on the upper lid an internal feedback mechanism can result in the muscles of the forehead contracting to raise the eye brow position in order to try to clear the skin off the lid - the reverse of the ‘roller blind’ effect. This can change not only the position of the eyebrow but also the shape of the eyebrow. When the excess skin is removed the drive to keep the eyebrows elevated ceases and the eyebrow assumes its natural shape and position seen when the forehead is relaxed (a simple demonstration of this is to take a video of yourself with your eyes open and then closed and noting how brow position changes once the forehead muscles relaxes).
Ptosis (drooping of the eyelid): The mechanism that opens the upper eyelid (known as the levator complex) is very delicate and can stretch with age. The muscles that are part of this mechanism may work harder than normal when the levator complex is stretched in an effort to keep the eyelid open in a normal position and this is especially the case when there is excess skin on the lid (there is an internal feedback system that stimulates the muscles to try to help the eyelid as open as possible). It may not be possible therefore to detect stretching of the levator complex prior to eyelid surgery. However, if the excess skin on the upper lids is removed the internal feedback system can be switched off causing the muscles to relax and the position of the upper lid to change (leading to a droopy appearance known as ptosis). This is not a complication of the surgery but unmasking of a pre-existing condition. If this does occur and you want to correct the ptosis, treatment involves surgery to retighten the levator complex.
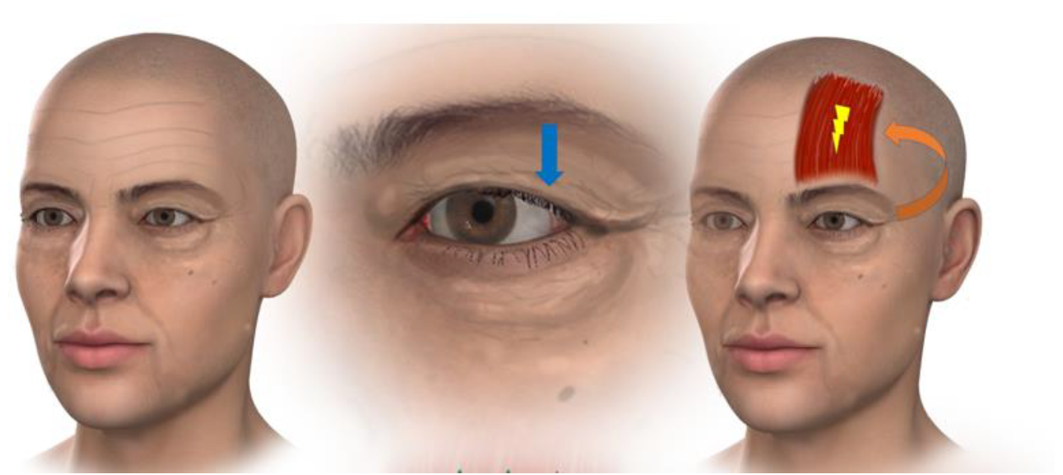
Left: With the ageing process excess skin gathers on the upper lid and the brow position descends, resulting in a change in the appearance of the eyelid (the skin on the eyelid itself is reduced or no longer visible) leading to a hooded appearance. This appearance is a combination of ‘true’ lid skin excess and brow descent. Middle: As the skin gathers on the lid the excess tissue places downward pressure on the lid (blue arrow). Right: Downward pressure on the lid produces an internal feedback loop which stimulates the frontalis muscle in the forehead.
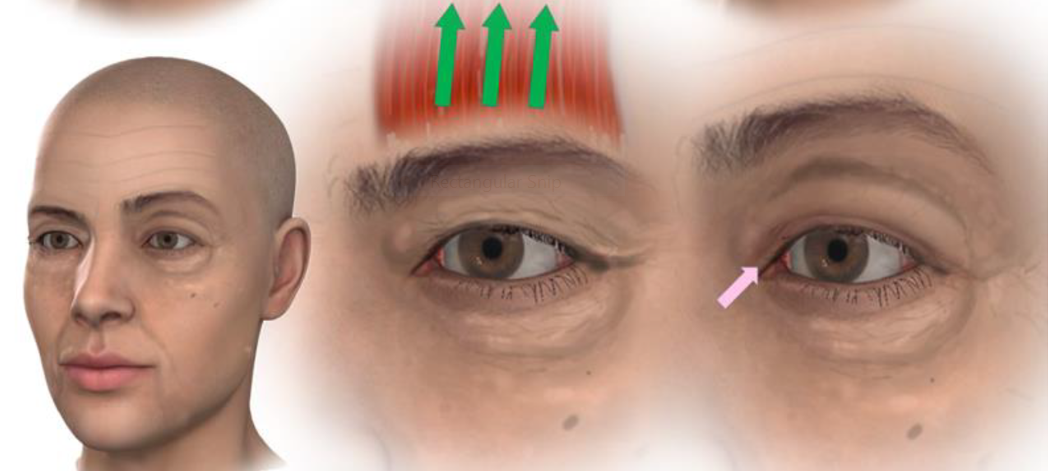
Left: Comparison of resting brow position (right side) and elevated brow position (left side). Middle: As the frontalis muscle is stimulated it elevates the eyebrow. Right: In the elevated position the eyebrow lifts some of the excess skin off the upper lid reducing the downward pressure on the lid. In the diagram the effect can be seen as some of the eyelid skin is revealed from beneath the fold of excess skin (pink arrow). The effect of the frontalis muscle contraction produces characteristic wrinkling of the forehead (these lines are often the target of muscle relaxing injections [into the frontalis muscle] which will result the brow position dropping leading to the sensation that the upper lid feeling heavier or less able to open as a result of the botulinum toxin administration – nothing has happened to the eyelid directly it is the indirect effect of the frontalis muscle not being able to maintain eyebrow position).
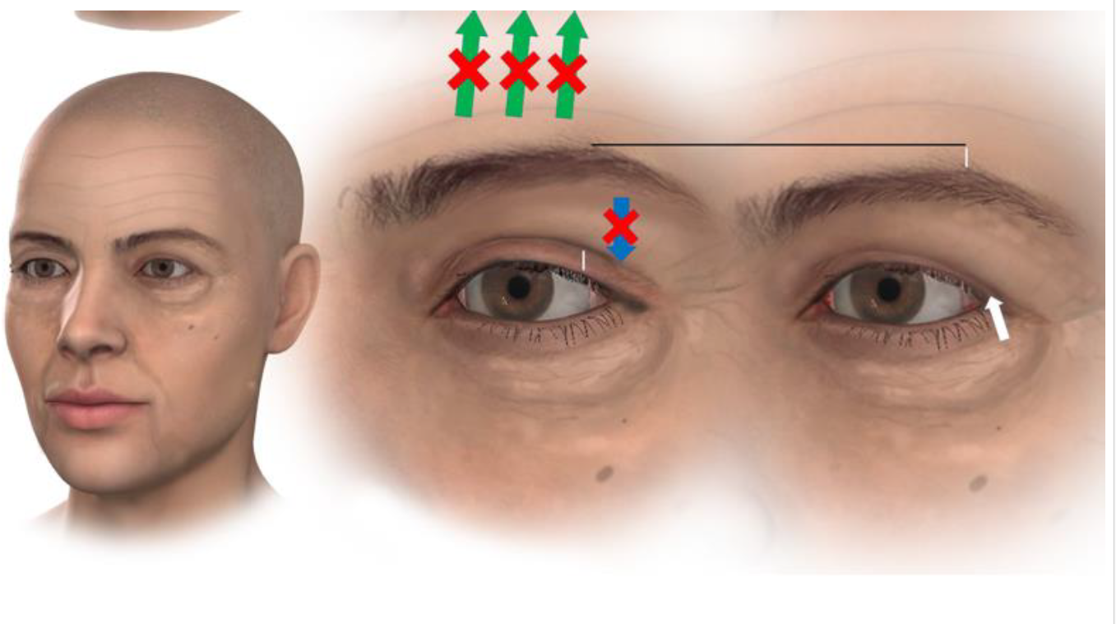
Left: The effects of a blepharoplasty can be seen comparing the right non operated side (excess skin on the lid, no visible eyelid skin) to the left operated side (eyelid skin visible) with both eyebrows sitting in lowered position (a brow lift not having been performed at the time of the blepharoplasty). Middle: After removing the excess skin from the upper lid following a blepharoplasty the downward pressure on the lid has been removed. The feedback loop keeping the frontalis muscle active is broken and the muscle relaxes. The amount of eyelid skin visible on the upper lid (shown by the vertical white line) is proportional to the amount of brow elevation produced by the frontalis muscle. Right: With the frontalis muscle relaxed the brow position drops (vertical white line above brow) and although the correct amount of skin has been removed from the upper lid by the blepharoplasty the amount of eyelid skin visible is reduced with the lid taking on a hooded appearance again (although in a less marked fashion). The typical appearance of this phenomenon is usually to produce a lateral hooding of the lid (denoted by the white arrow) as the lateral portion of the brow usually descends the most with the loss of frontalis muscle action.
COMPICATIONS AND RISKS OF SURGERY
Anyone considering surgery should approach the decision with a healthy amount of respect and caution, especially when the surgery is elective (or planned) and is non-essential surgery (as aesthetic or cosmetic surgery generally is).
All surgical procedures have limitations in terms of achievable outcomes and it is important that your expectations match what is possible through surgery and that you are aware of the material risks and complications. Your surgeon will have discussed these risks and complications during your consultation. It is important that you take the time to read them prior to your next consultation.
GENERAL COMPLICATIONS / RISKS
Bleeding: It is possible, though unusual, to experience a bleeding episode during or after surgery. Should post-operative bleeding occur, it may need draining surgically. If a collection of blood accumulates within the upper eyelid (a haematoma) this may need draining. The problems that can be encountered as a result of a haematoma in the eyelid include skin discolouration, skin necrosis (skin death caused mechanically due the pressure effect of the fluid collection or by the release of chemicals from the break down products of the blood clot). In extreme cases a collection of blood that occurs inside the eye socket itself can result in pressure on the eyeball and the nerve to the eyeball (the optic nerve) resulting in blindness (this would necessitate an emergency return to theatre to drain the haematoma and relieve the pressure on the optic nerve and eyeball).
Seroma: A seroma can be best thought of a collection of fluid beneath the skin or within the tissue at a surgical site. If this occurs there is the possibility it will need to be drained with a needle, it may resolve itself or require an operation to drain it.
Infection: Infection is unusual after surgery. Should an infection occur, additional treatment including antibiotics, hospitalisation, or additional surgery may be necessary. In very rare cases a significant infection of the facial tissues can occur (known as orbital cellulitis) which can be life threatening.
Scarring: All surgery leaves scars, some more visible than others. Although good wound healing after a surgical procedure is expected, abnormal scars may occur within the skin and deeper tissues. Scars may be unattractive and a different colour compared to the surrounding skin. Scar appearance may also vary within the same scar. Scars may be asymmetrical (appear different on the right and left side of the body). There is the possibility of visible marks in the skin from sutures. In some cases, scars may require surgical revision or treatment. Scars can appear thick, red and raised all or part of the way along the incision line (a hypertrophic scar) or more rarely can involve tissues beyond the incision itself (and can resemble a badly healed burn), this is known as a keloid scar. Additionally, scars can tether to underlying structures or become abnormally pigmented. It is possible that additional treatments may be required for adverse scarring.
Delayed Healing: Wound disruption or delayed wound healing is possible. Some areas of the treated region may not heal normally and may take a long time to heal. Areas of skin may die. This may require frequent dressing changes or further surgery to remove the non-healed tissue. Individuals who have decreased blood supply to tissue from past surgery or radiation therapy may be at increased risk for delayed wound healing and poor surgical outcome as many patients with conditions such as diabetes. Smokers have a greater risk of skin loss and wound healing complications.
Skin Discoloration / Swelling: Some bruising and swelling normally occurs following surgery. The skin in or near the surgical site can appear either lighter or darker than surrounding skin. Although uncommon, swelling and skin discoloration may persist for long periods of time and, in rare situations, may be permanent. Additionally, these areas may have exaggerated responses to hot or cold temperatures. Because of changes in the pattern of blood flow within the face brought about by the surgery it is possible to develop new blood vessels which may be visible under the skin.
Sensory changes: With any form of surgery small nerve branches that supply the skin will be cut. This can lead to patches of numbness around the surgical site. It is possible that, following surgery, you can develop abnormal sensation in the area where you have had surgery and this may take the form of pins and needles (known as paraesthesia), hyper sensitivity or even pain in response to normal touch and further surgery may help. It may be necessary to take medication to control any such symptoms on a permanent basis. Numbness following surgery is normal and usually resolves after 9 to 12 months (known as allodynia). Such problems may be related to nerves becoming entrapped within scar tissue.
Suture extrusion: Eyelid skin is very thin and does not normally require deep stitches (sutures) to be used as part of the wound closure. However, in certain circumstances your surgeon may need to use sutures on the deeper tissues. These sutures are usually made out of material which is broken down by the body – often called dissolving sutures although sometimes a long lasting (or even permanent) suture may be needed. It is possible that you may develop redness in an area of the incision that is fully healed (3 or more weeks following surgery) and it appears that pus comes out. This is the body’s response to a deep stitch and the ‘pus’ represents the white blood cells trying to dissolve the suture (causing localized inflammation but without infection). Such areas are normally managed with simple dressings. It is possible to develop multiple suture extrusions at the same time or at different times during the healing process.
Allergic Reactions: Local allergies to tape, suture material and glues, blood products, topical preparations or injected agents can cause skin reactions. Serious systemic reactions including shock (anaphylaxis) may occur to drugs used during surgery and prescription medications. Allergic reactions may require additional treatment and can result in severe illness or death. Often, they result in minor irritation/ discomfort and resolve reasonably quickly.
Deep vein thrombosis, cardiac and pulmonary complications: Any procedure requiring general anaesthesia increases the risk of the formation of blood clots in the legs. Such clots can dislodge and move to the lungs, causing shortness of breath and strain on the heart. Such clots can potentially be fatal. If you experience shortness of breath, chest pains or palpitations (abnormal heart beats) following your surgery it is important you seek medical advice immediately.
Blood Transfusion: Blood loss during surgery may require treatment with a blood transfusion. It is possible for viral transmission to occur with such treatment (HIV, hepatitis, and others). Having a blood transfusion can result in a transfusion reaction that can cause serious illness.
COMPLICATIONS SPECIFIC TO UPPER LID BLEPHAROPLASTY SURGERY
Skin necrosis: If the blood supply to the skin is insufficient following surgery (which can be for a variety of reasons) it can necrose (die). If this happens the skin will form an eschar (scab) which may need to be removed surgically. Dressings are likely to be required for a period of time and further surgery may be needed to correct adverse scars.
Fat necrosis: If the fat cells beneath the skin or within the eye socket itself have inadequate blood supply or are traumatised by manipulation during the procedure that will result in the tissue dying. This can result in the formation of lumps beneath the skin which may be felt and, in some circumstances, seen. Discharge of liquid from the surgical incision is possible due to fat liquification. Additional surgery to remove areas of fat necrosis may be necessary. If an area of fat necrosis were to become infected it would require further treatment with antibiotics or surgery. There is the possibility of contour irregularities in the skin that may result from fat necrosis.
Skin Contour Irregularities: Contour and shape irregularities may occur after upper lid blepharoplasty surgery. Visible wrinkling or puckering of the skin may occur and may require additional treatment if problematic. Any fluid collections that occur beneath the skin can also lead to contour irregularities and may require additional treatment.
Dry eyes and the need for eye drops: As part of the surgery the excess skin on the upper lid (as well as the deeper eyelid tissues) are treated in order to produce a change in appearance. For some patients that can result in limitations of movement. Under normal circumstances the eyelids are soft and the small muscles that move them are able to make the lids move quickly (when we blink). Following blepharoplasty surgery the eyelids will become swollen and stiff. For some individuals the speed at which the eyelids can close is reduced - leading to eyes feeling dry and requiring the use of eye-drops. This is usually only a temporary phenomenon, however in those who have a tendency towards dry eyes in the first place, the sensation of dryness can be long lasting and lubricating eye drops may be required on a permanent basis.
Motor nerve injury: There is the potential for injury to the nerves that surround the eye socket. The ability to raise your eyebrows or close your eyes may be affected as a result of this. This can produce weakness of the affected muscles (and asymmetry of movement between sides of the face) or paralysis (resulting in complete loss of movement in the affected region). Any such deficit is likely to be temporary (resolving in a few weeks to months) but may be permanent.
Sensory nerve injury: There are 2 sensory nerves that are associated with the upper eyelid, running out of the upper aspect of the eye socket and providing sensation to the skin of the forehead (the supraorbital and supratrochlear nerves). These nerves may be damaged as part of upper lid surgery producing altered sensation in the forehead (this can take the form of numbness, pins and needles or even pain). Such changes may be temporary or permanent.
Inability to close the eyelid: If too much skin is removed it may not be possible to fully shut the eye and a further operation would be required to graft additional skin onto the eyelid to rectify the situation. Such limitations usually resolve within a few months of the surgery but some patients may experience a persistent feeling of restriction.
Double vision: The small muscles that move the eyeball are located within the eye socket itself. A rare complication of eyelid surgery is damage to these muscles. If the muscles are damaged this may lead to reduced movement of that muscle and loss of synchronisation of eye movement, this would result in double vision. If this occurs it usually resolves spontaneously but, in some cases, may require surgery to correct it.
Corneal abrasion: The eyeball has a delicate surface which can be grazed or scratched by touching it. During surgery if a swab or an instrument rub against the eyeball it is possible to cause such a graze (medically termed an abrasion). Although such abrasions (which can be painful) will normally heal quickly by themselves, additional treatment may be required in the form of regular eye drops, the use of a temporary eye patch or even a temporary stitch to hold the eye shut.
Corneal ulceration: If the delicate surface of the eyeball dries out (because the eyelids are not able to fully shut following surgery - which is often the case - or because the ability to blink is reduced - also often the case) the eyeball can develop an ulcer (this can be painful). If this occurs additional treatment may be required in the form of regular eye drops, the use of a temporary eye patch or even a temporary stitch to hold the eye shut.
ASYMMETRY OF THE EYELIDS AND ORBITS
Everyone is different on the right-hand side of their face compared to the left and pre-existing asymmetry between sides will influence the outcome of your surgery.
Particular areas of asymmetry frequently seen include:
Facial bone asymmetry: The size, shape and position of the facial bones are inherently asymmetric. This is particularly noticeable in the location of the orbits (eye sockets) and it is not unusual for the eye sockets to have different degrees of tilt (the outer corner of the eye appearing higher or lower than the other side - technically known as canthal tilt).
Skin fold and wrinkle asymmetry: The muscles in the face will have different directions of pull and will produce different amounts of force. This will produce differences in the skin folds and wrinkle pattern seen between the sides of the face both before and after surgery. In relation to eyelid surgery this is particularly relevant to the wrinkles on the side of the temple known as ‘crow’s feet’. On the lid itself, the skin crease used as the marker for the lower part of the skin incision (the supratarsal crease) is often a slightly different distance from the lid margin meaning that the position of the scars may vary between the eyelids.
Volume asymmetry: The shape and contour of the eyelid and eye socket may differ between sides following surgery.
Scar asymmetry: The shape, length and position of the scars between the right and left sides of the face may be different.
SPECIFIC HEALTH FACTORS AFFECTING THE OUTCOME OF BLEPHAROPLASTY SURGERY
Body mass index: Research has shown that the higher your body mass index (BMI) the more likely you are to have a complication post-surgery. Achieving the healthiest BMI possible prior to surgery is always recommended.
https://www.nhs.uk/live-well/healthy-weight/bmi-calculator/
Smoking: Smoking or vaping with a nicotine vape (or using a nicotine patch or gum) reduces blood flow to the tissues and results in poorer scarring, wound healing and is associated with a higher rate of complications in general. You are advised to stop smoking 6 weeks prior to surgery and to refrain from smoking thereafter.
Medications: Certain medications can interfere with wound healing and increase the likelihood of infections following blepharopasty surgery. It is important that you inform your surgeon of all the medications you are on.
Diabetes: Diabetes affects immune system function, as well as tissue perfusion (blood flow) and wound healing. You are at higher risk for developing complications following surgery if you suffer with diabetes.
ADDITIONAL CONSIDERATIONS RELATING TO BLEPHAROPLASTY SURGERY
Surgical plan: Although a pre-operative plan will have been discussed prior to the operation, there are multiple ways of undertaking an individual procedure. Each technique has been developed to achieve the same end result (though may result in differing scar patterns). It may sometimes be necessary to alter the initial plan discussed with you at the time of operation due to anatomic considerations that become apparent during the course of the surgery. Your surgeon will discuss with you what may be subject to change or what these changes may be - this varies between different types of procedure.
Unsatisfactory Result: Although good results are always aimed for, they cannot be guaranteed. You may be disappointed with the results of your blepharoplasty surgery. Asymmetry between sides of the face, loss of function, wound disruption, poor healing, and loss of sensation may occur after surgery. Unsatisfactory surgical scar location or visible deformities at the ends of the incisions (dog ears) may occur. The long term results of the surgery are dependent on tissue quality scar tissue formation (these factors cannot be controlled as part of the surgery) and insufficiency of these factors can result in early loss of tissue position and recurrence of skin sag.
Although the risks and complications occur infrequently, the above risks are particularly associated with blepharoplasty surgery. In addition to the risks and complications outlined above there are others that can and do occur, though these are even more uncommon. The outcomes of surgery and medicine are influenced by many factors beyond the control of your surgeon and as such cannot be predicted.
Disclaimer:
This website is designed to supply useful information but is not to be regarded as advice specific to any particular case. It does not replace the need for a thorough consultation and all prospective patients should seek the advice of a suitably qualified medical practitioner. The BAAPS accepts no liability for any decision taken by the reader in respect of the treatment they decide to undertake.
